What’s new in UC: UEGW ’24 and ECCO ‘25
DISEASE CLEARANCE, RESPONSE PREDICTION AND TREATMENT PERSISTENCE IN UC
Clinical studies on the effectiveness of therapies for UC often use endpoints that include clinical or endoscopic remission, but histological remission is also increasingly reported. Achieving the combination of these endpoints in one and the same patient is called disease clearance (DC)1, but evidence on whether pursuing such strict treatment targets will result in a significant benefit to patients is currently lacking. In addition, it is important that patients can maintain their treatment outcomes for as long as possible.
During the past congresses, several abstracts were presented that are very relevant in the context of these questions. In this communication we would like to bring a selection of some abstracts in the spotlight.
Disease clearance in UC: main takeaways
UEGW 2024 brought us the interim results of clearance week 32 of the VERDICT randomized controlled trial2, and ECCO 2025 added the interim results of week 484 . The VERDICT trial investigates whether applying the stricter treatment target of DC leads to a more favorable outcome week for UC patients.
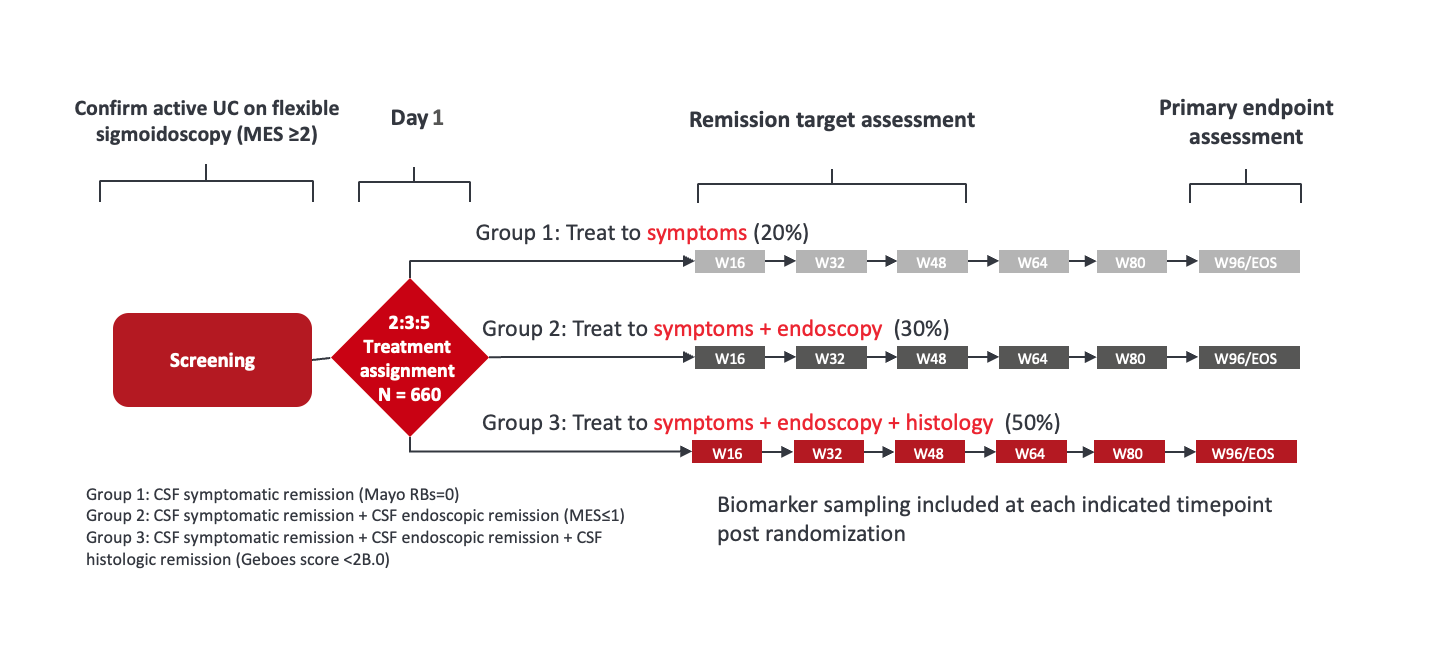
Figure 1. VERDICT study design. Adapted from Jairath et al. 20242
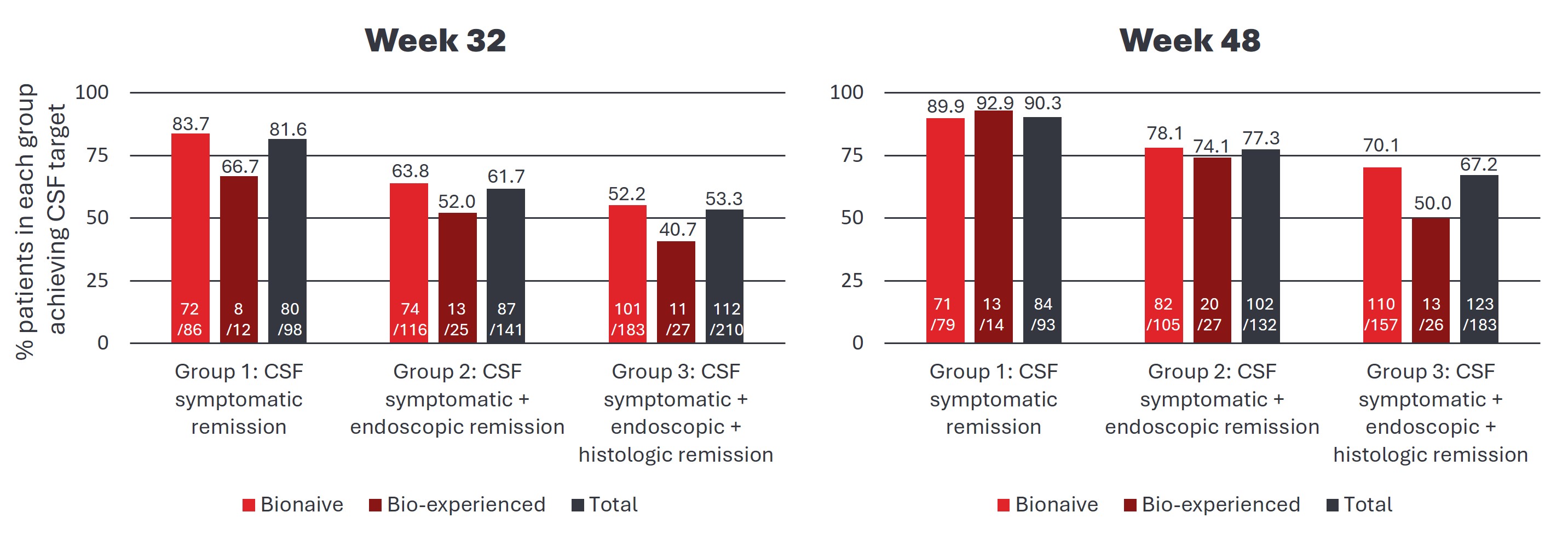
Patients were randomized into three groups (see Fig 1), with each group having to meet increasingly strict treatment targets. The three arms and their respective treatment targets were defined as follows: 1) CSF symptomatic remission (Mayo rectal bleeding subscore = 0), 2) CSF symptomatic remission and endoscopic remission (Mayo Endoscopic Score [MES]≤1), and 3) CSF symptomatic remission and endoscopic remission and histologic remission (Geboes score<2B.0). In the patients who reached their week 32 or week 48 visit, the proportion of patients in the three groups who achieve remission is as follows (Figure 2).
Figure 2. Remission in patients with as observed data at the week 32 (left) and week 48 (right) study visit. Adapted from Jairath et al. 20242 and Jairath et al. 20254
This interim analysis of the as observed data shows that the strict target of CS-free symptomatic and endoscopic and histological remission was achieved in 70.1% of the bio-naïve patients, and 50% of the bio-experienced patients who had reached their week 48 visit.
After the completion of the VERDICT study, which will run for a total of two years, it will become clear to what extent patients benefit from the use of such stricter treatment targets.
Although it has not been formally demonstrated that disease clearance leads to better results in the long term, there is increasing interest in this outcome.
A post-hoc analysis of the mirikizumab LUCENT-UC studies (the pivotal phase 3, randomized, double-blind, placebo-controlled trials of mirikizumab) reported the number of patients in CS-free remission, depending on whether they achieved DC at week 12. It showed that 59.1% of the patients who achieved DC under mirikizumab at 12 weeks were in CS-free remission after 1 year, while 40.1% of patients who did not achieve mirikizumab DC at 12 weeks were in CS-free remission after 1 year3. In a Spanish prospective longitudinal cohort (n = 101), which included UC patients with and without anti-TNF treatment, it was also found that patients who achieved DC had a lower risk of negative outcomes (defined as need for therapy or escalation of treatment, hospitalization or colectomy) (Fig 3)5. An Argentinian etrospective cohort study (n = 197) found that the combination of a Mayo Endoscopic Subscore of 0-1 and a Nancy Index of 0-1 was associated with better outcomes than achieving only one of these parameters6.
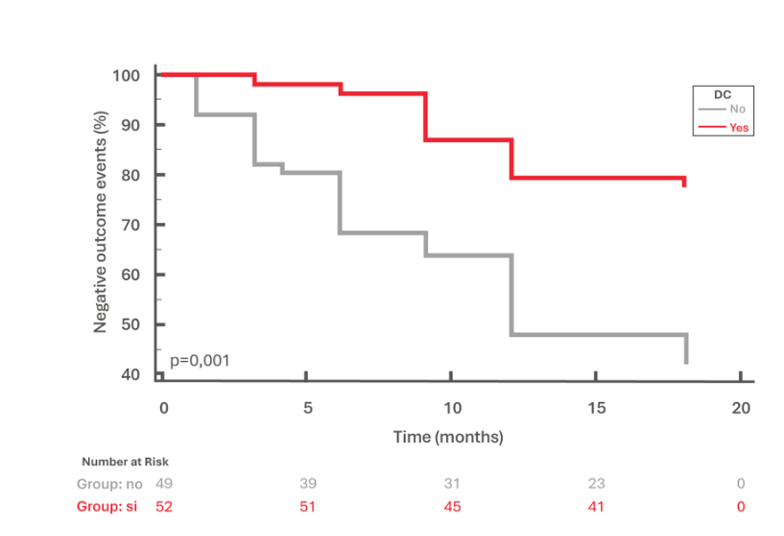
Figure 3. Survival curve for the risk of recurrence depending on whether disease clearance was achieved or not. Adapted from Ramos Lopez et al. 20255
This supports the concept that reaching DC (early) can lead to better long-term outcomes, but the only study that has truly been designed to formally demonstrate it is the VERDICT trial… Stay tuned!
VDZ treatment and treatment effect persistence: main takeaways
- Several studies report a VDZ treatment persistence of more than 70% after 1 year9-12
- After 2 years, treatment persistence was 64.2% in a meta-analysis9, and 73.3% in the RUN-UC study12
UEGW and ECCO provided us with numerous abstracts describing long term outcomes. A meta-analysis of real-world data (publication date 2014-2022) examined treatment persistence under VDZ9. This was found to be 72.4% (95% CI 68.7-75.8) after 1 year,and 64.2% (95% CI 55.3-72.2) after 2 years of VDZ. In the included studies, it was found that treatment persistence after 1 year did not differ between bio-naïve and bio-experienced patients: 74.5% (95% CI 66.8-80.9) and 73.1% (95% CI 62.4-81.6) respectively. In this meta-analysis, 42.7% (95% CI 38.4-47.1) of treated patients achieved CS-free clinical remission after 1 year, and in the 29 studies where mucosal healing was reported, 42.6% (95% CI 37.0-48.3) were found to have achieved this endpoint. No safety data was reported in this study, but a second meta-analysis of studies that reported efficacy and treatment patterns of VDZ and anti-TNF in bio-naïve patients did report safety data. In the included studies, serious adverse events (SAE) were reported for VDZ in 4.5%, 6.8% and 14.3% of VDZ-treated patients, while in the same studies, 5%, 19.2% and 10.9% of anti-TNF-treated patients reported SAEs, respectively.10
At ECCO, a Canadian study reported on the efficacy and persistence of second-line treatment with VDZ (n = 122) and UST (n = 28) after anti-TNF11. In this cohort, 82.3% of VDZ-treated patients were in clinical remission at 12 months, with 91.5% treatment persistence . In terms of safety, infections were reportedin 4.1% of the patients in the VDZ group, with no serious adverse events reported for either VDZ or UST. The German prospective, controlled, propensity score-adjusted RUN-UC study included patients treated with UST (n = 153), anti-TNF (n = 165) and VDZ (n = 165). This study reported a VDZ persistence of 73.3% and clinical remission of 48% (and 43.9% in bio-experienced patients) after two years of follow-up12.
For a complete overview of all abstracts presented, please refer to the abstract books: UEG 2024 and ECCO 2025.
Taken together, UEGW 2024 and ECCO 2025 showed that important steps being taken in determining the right treatment targets in UC, and we can look forward to the results of this in the coming years. In addition, the efficacy, high treatment persistence and safety profile of vedolizumab were confirmed.
†Chi-Square test comparing three therapy groups. *Adalimumab: 30.3%, infliximab: 61.8%, golimumab: 7.9%.
UEGW: United European Gastroenterology Week, ECCO: European Crohn’s and Colitis Organization, UC: ulcerative colitis, CS: corticosteroid, VDZ: vedolizumab, DC: disease clearance, CD: Crohn’s disease, TNF: tumor necrosis factor, SAE: serious adverse events, ; mITT: modified intention-to-treat; PS: propensity score, UST: ustekinumab
REFERENCES
1. Danese S, et al. Nat Rev Gastroenterol & Hepatol. 2020; 17:1-2; 2. Jairath V, et al. United European Gastroenterol J. 2024; 12(S8):978-979; 3. Colombel JF, et al. United European Gastroenterol J. 2024; 12(S8)582-583; 4. Jairath V, et al. J Crohns Colitis 2025; 19(S1):i180-i181; 5. Ramos Lopez L, et al. J Crohns Colitis 2025; 19(S1):i236-237; 6. Marturano MV, et al. J Crohns Colitis 2025; 19(S1):i2160; 7. Sands BE et al. N Engl J Med. 2019; 381(13):1215-1226 8. D’Haens GR et al. United European Gastroenterol J. 2024; 12(S8):129-130; 9. Chaparro M, et al. United European Gastroenterol J. 2024; 12(S8):966; 10. Vermeire S, et al. United European Gastroenterol J. 2024; 12(S8):977; 11. Jairath R, et al. J Crohns Colitis 2025; 19(S1):i1185; 12. Bokemeyer B, et al. J Crohns Colitis 2025; 19(S1):i2127-i2128.
smpc
price