
THE VDZ-CDST SCORING SYSTEM: BACKED BY A GROWING BODY OF EVIDENCE
The VDZ-CDST scoring system has been developed and tested through post hoc analyses using data from over 2400 patients across multiple cohorts from studies conducted globally.
TREATING THE RIGHT CD PATIENT AT THE RIGHT TIME
Crohn's disease is a progressive disease, and it is important to get patients into deep remission early in their disease course. One of the most important questions here is how quickly after diagnosis a patient should be treated with advanced therapy, if conventional therapy proves insufficient. At both UEGW 2024 and ECCO 2025, it was once again underlined that the answer to this question is undoubtedly "as soon as possible". However, we are also confronted with heterogeneity in clinical outcomes: even when treating patients early with advanced therapies, there is no one-size-fits-all solution1. There is therefore an increasing focus on personalizing treatments, with a strong focus on identifying strategies to predict a patient's likelihood of response.
Several abstracts were presented that are very relevant in the context of these questions. On this page, we would like to highlight some of them.
Early treatment in CD: main takeaways
At UEGW 2024, the final results of the LOVE-CD study were presented2. This prospective, open-label study included 260 patients in Belgium, the Netherlands and Hungary in two groups:
'Early CD’ was defined as a disease duration of <2 years and naïve to therapy or only treated with corticosteroids and/or immunomodulators (n = 86).
'Late CD’ was defined as a disease duration of >2 years and exposure to corticosteroids, immunomodulators and anti-tumor necrosis factor (TNF) (n = 174).
Both groups were treated with intravenous VDZ (300mg) at weeks 0-2-6 and every 8 weeks after that for a total of 52 weeks. A week 10 infusion was given if patients did not achieve a drop in CDAI of at least 70.
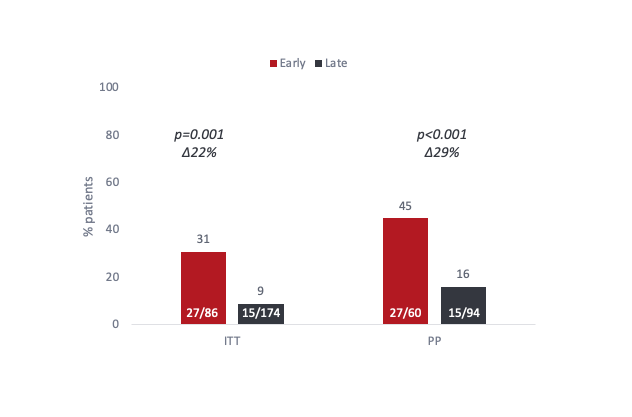
Figure 1. Proportion of patients meeting the primary endpoint of clinical and endoscopic remission (CDAI ≤150 and SES-CD <4) at W26 and W52. ITT = Intention to treat, PP = per protocol. Adapted from D’Haens et al. 2024
When we look at the (strict) primary endpoint of clinical and endoscopic remission (Crohn's disease activity index (CDAI)≤150 and Simple Endoscopic Score for Crohn's Disease (SES-CD) <4)) at both weeks 26 and 52 in these two groups, we see that patients from the early CD group do significantly better than patients from the late group (Figure 1). At ECCO, an additional analysis was presented that shows a difference in CS-free.
The key secondary endpoints of the LOVE-CD trial, such as endoscopic response and remission showed a similar picture, with higher efficiency of vedolizumab (VDZ) for the early CD group compared to the late CD group2.
5% of early CD patients treated with VDZ reported severe AEs, while in the group of late CD patients treated with VDZ this was 27% (p<0.0001). The reported serious AEs in the early vs late groups include infection (1.2 vs 7.5%), bowel obstruction (0 vs 2.3%), CD flare (2.3 vs 4%), abdominal pain (0 vs 1.7%) and malignancy (0 vs 1.7%)2.
Another relevant question in Crohn’s disease is whether there are differences in healing rates of the ileum and the colon. A previous analysis of the LOVE-CD data at ECCO 2024 found no significant differences in endoscopic remission when patients were stratified according to disease location5. At ECCO 2025, the researchers investigated this even deeper and compared histological healing rates in 336 colon and 114 ileum biopsies taken from 179 patients at week 26, and 323 colon and 112 ileum biopsies taken at week 52. Histological assessment confirmed the efficacy as assessed by endoscopy, with 38.5% of patients with early CD achieving histological healing, which was significantly higher than the late CD group (14.9%, p=0.00004). When comparing colon and ileum, endoscopic remission, histo-endoscopic mucosal improvement (HEMI; Geboes score ≤3B.1) and histo-endoscopic mucosal remission (Geboes score <2B.1) rates were similar across the two locations (Fig 2).
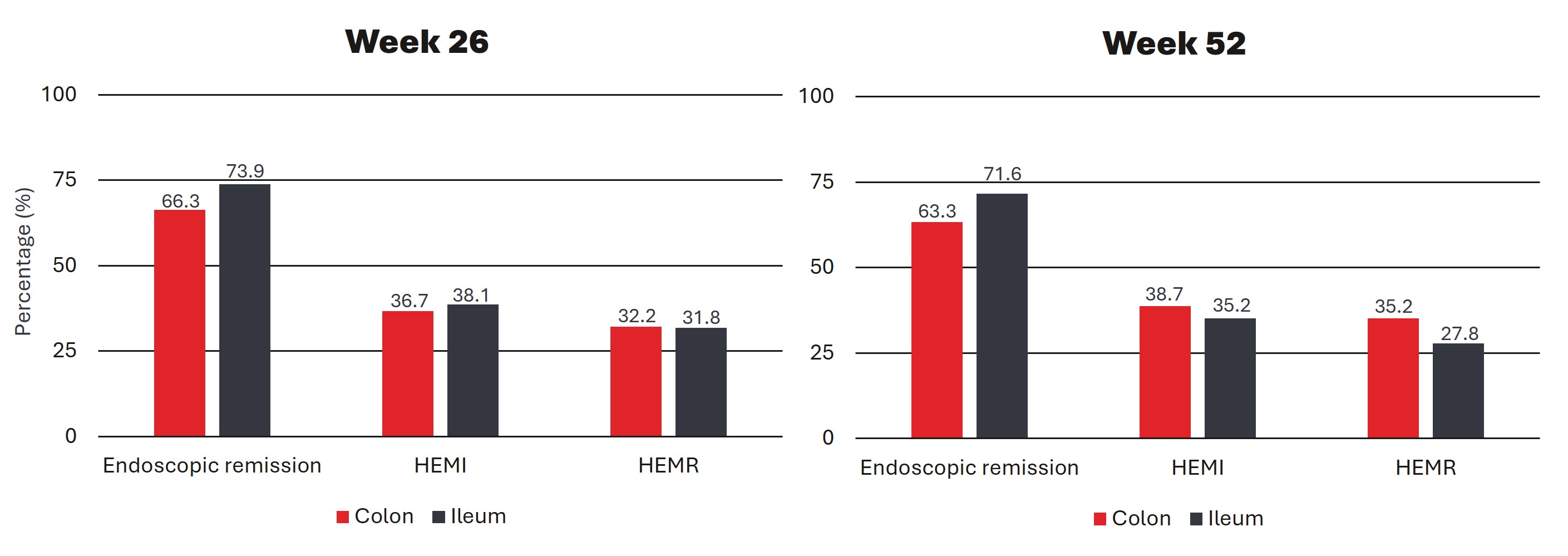
Figure 2. Rates of endoscopic remission, HEMI and HEMR at week 26 and week 52 stratified by disease location.
Adapted from Lenfant et al4
The VDZ-CDST: main takeaways
The VDZ-CDST was first described in 20188. Based on 5 clinical parameters, patients can be divided into groups that have a low, intermediate or high probability of response for VDZ (Fig 3).
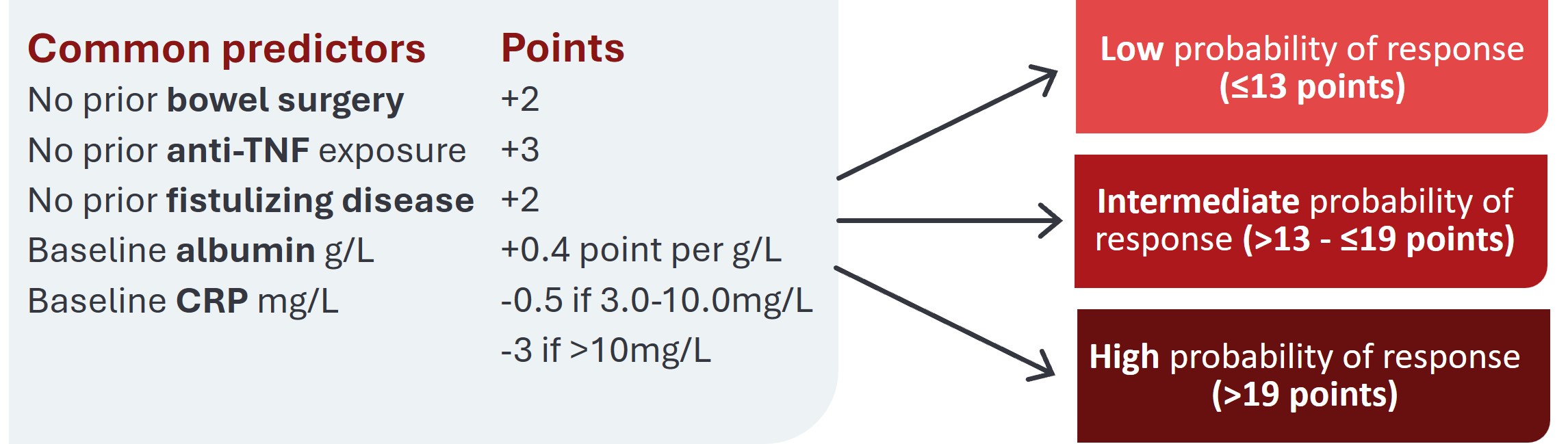
Figure 3. The five parameters of the VDZ-CDST. Adapted from Dulai et al. 20188
At UEGW, an abstract was presented in which the VDZ-CDSTVDZ-CDST was retrospectively tested on a cohort of 130 British patients from a single tertiary center6. This cohort included 9 patients with low, 51 with medium and 70 with high probability of response. The authors found that the group with a high probability of response showed superior responses. The main endpoint of treatment persistence was 56%, 69% and 80% for patients with low, intermediate and high probability of response, respectively (p = 0.048) (Fig 4, left). In patients for whom mucosal healing (MH, defined as absence of ulcerations) data was available after 12 months of treatment, a similar effect was seen: in the low group 20% of the patients showed MH, in the intermediate group 46% and in the high group 76% (p = 0.0023, Fig 4 right). Additionally, the authors found a difference in progression to surgical interventions, in favour of the group of patients with a high probability of response. 16% of patients in the high probability of response group underwent surgery, while for the low and intermediate groups this was 33% and 31 respectively (p=0.042).
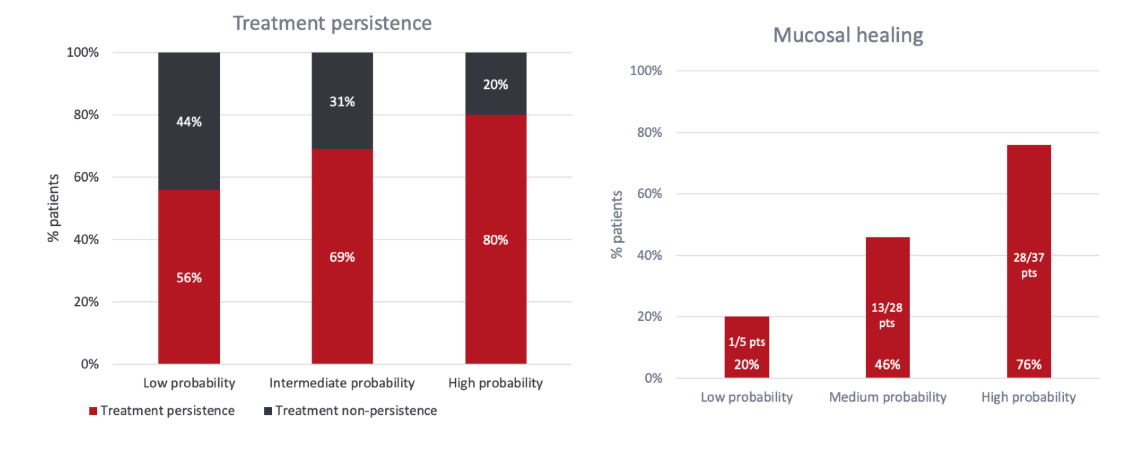
Figure 4. Left. Treatment persistence. Right. Percentage of patients with mucosal healing at 12 months.
Adapted from Choon et al. 20246.
At ECCO, this analysis was further expanded to include patients starting VDZ between January 2015 to October 2023 in two tertiary IBD centres and now also included patients receiving subcutaneous (SC) VDZ. In this analysis, the high probability group demonstrated higher treatment persistence in both the IV (n=278) and SC (n=130) subgroups7. Additionally, higher rates of mucosal healing were observed in the high probability groups when compared to the low/intermediate group.
Taken together, UEGW 2024 and ECCO 2025 confirmed that early treatment is crucial in CD. Additionally, it is possible to gain some insight into which patients are most likely to have a more favourable disease course under VDZ treatment with the support of the VDZ-CDST.
For a complete overview of all abstracts presented, please refer to the abstract books: UEG 2024 and ECCO 2025.
CDAI: Crohn’s disease activity index, CD: Crohn’s Disease, ITT: Intention-to-treat, PP: per protocol, VDZ-CDST: vedolizumab clinical decision support tool, MH: mucosal healing, SES-CD: Simple Endoscopic Score for Crohn’s Disease, TNF: tumor necrosis factor, QALY: quality-adjusted life-years, IV: intravenous; SC: Subcutaneous; UEGW: United European gastroenterology week; ECCO: European Crohn’s and Colitis Organization
REFERENCES
1. Noor NM, et al. Lancet Gastroenterol Hepatol. 2020; 5(1):80-92. 2. D’Haens GR, et al. United European Gastroenterol J. 2024; 12(S8):129-130; 3. Oldenburg L, et al. J Crohns Colitis 2025; 19(S1):i240-241; 4. Lenfant M, et al. J Crohns Colitis 2025; 19(S1):i177-179; 5. Hens B, et al. J Crohns Colitis 2024; 18(S1):i1560- i1561; 6. Choon XY et al. United European Gastroenterol J. 2024; 12(S8):595; 7. Choon XY, et al. J Crohns Colitis 2025; 19(S1):i1595- i1596; 8. Dulai PS et al. Gastroenterology. 2018; 155(3):687-695.e10.
C-APROM/BE/ENTY/0276 – March 2025
The VDZ-CDST scoring system has been developed and tested through post hoc analyses using data from over 2400 patients across multiple cohorts from studies conducted globally.
There is a growing need to shift from 'reactive' management driven by disease complications to 'proactive' care with the aim to prevent disease damages.